11.1 Changes in the Demand for Health Services
As indicated, SWSAHS’s population is projected to grow by 13.7% from 731,615 in 1996 to 830,509 in 2006. Population growth and ageing are the two main factors in rising demand for health services.
NSW Health’s Activity Projections Plus Interventions (APPI) model predicts a 4% per annum growth in acute inpatient activity from 1996 to 2001. This is due to a range of factors including population growth and ageing and trends in acute service provision. APPI makes forecasts for 98% of SWSAHS’s current hospital separations and 83% of SWSAHS’s current hospital bed days. APPI excludes acute psychiatric activity. Acute psychiatric and non acute cases in hospitals account for 2% of all separations but 17% of all bed days.
Table 9 summarises the estimated projected demand for a range of services for SWSAHS residents to 2006. More detail on the demand projections is provided at Appendix E.
Demand in this context refers to the requirement for health services from the community based on models which consider trends from current and past service utilisation, population growth and ageing and anticipated changes in the provision of services. SWS resident’s demand can be met through access to services provided within SWSAHS, by other Area Health Services or interstate.
It should be noted that this represents a forecast of the future activity based on a number of assumptions, including no change in the current flow of patients and trends in acute services utilisation.
Interpreting these forecasts requires some cautionary notes. The forecasts are based on observed trends from 8 prior years of data. Regression analysis is a statistical method of predicting forward but it does not by itself design the future.
The main issues arising from the forecasts of activity in Table 9 are:
- An increase in the demand for services;
- Reductions in the length of stay for acute services;
- There is no agreed methodology for estimating demand for non acute, mental health, non inpatient and community based services. Data on utilisation of services in other Area Health Services for non inpatient and community is not available.
Table 9 - Estimated Demand 1996-2006
Acute Hospital Resident Demand (APPI) in all Hospitals in NSW and Interstate |
||||
1996/7 |
2001 Forecast | 2006 Forecast | Change 1996-2006 | |
| Separations | 135,500 |
163,668 |
193,350 |
43% |
| Bed days | 490,007 |
502,472 |
522,709 |
6.7% |
| Average LOS | 3.6 |
3.1 |
2.7 |
-25% |
| Statewide beds required (90% occupancy) | 1,492 |
1,530 |
1,591 |
+99 |
Non Acute Hospital Resident Demand in all Hospitals in NSW |
||||
| Separations | 3,059 |
3,670 |
4,313 |
41% |
| Bed days | 64,914 |
73,400 |
81,947 |
24% |
| Average LOS | 21.2 |
20 (assumed) | 20 (assumed) | -1.2 |
| Statewide beds required (95% occupancy) | 187 |
212 |
236 |
+50 |
Acute Psychiatric Resident Demand in all Hospitals in NSW |
||||
| Separations | 3,214 |
3,857 |
4,532 |
41% |
| Bed days | 28,502 |
34,327 |
40,335 |
41% |
| Average LOS | 8.9 |
8.9 (assumed) | 8.9 (assumed) | 0 |
| Statewide beds required (90% occupancy) | 87 |
104 |
122 |
+35 |
Non Inpatient Resident Demand |
||||
| ED Attendances | Total SWS resident demand for non inpatient services is not known as information on SWS attendances at other Area Health Services is not available | |||
| ED Admissions | ||||
| NAPOOS | ||||
Community Based Resident Demand |
||||
| Occasions of Service | Total SWS resident demand for community based services is not known as information on SWS attendances at other Area Health Services is not available | |||
Whether the forecast increase in demand for acute services becomes a reality will largely depend on funding being available to treat more patients. However, there may not be funding to match the forecast demand growth or SWSAHS may choose to invest future growth money in non inpatient care or in population health prevention initiatives. This will increase queues for non urgent conditions and a continued skewing of expenditure towards acute urgent care. Attendances at Emergency Departments may increase as queue avoidance is practiced. Under conditions of rising demand and possibly constrained resources, rules for prioritising allocation of funds become essential. Without some plan to control this or place limits, expenditure will be most influenced by urgency and less influenced by value for money, that is, what expenditure does most to ameliorate the burden of disease.
The importance of having strategies that deal with forecast rising demand cannot be over emphasised. It may not actually be necessary to treat all the rising demand. For example, earlier intervention and prevention strategies may reduce future demand for services and better management of chronic illness may prevent or reduce admissions. Expenditure needs to rationed in a systematic fashion and with a view to achieving best value for money.
The ability to triage and redirect care to less costly but equally effective settings from Emergency Departments will become essential. Current emergency services are tuned to triage and effective management of urgent care with providers focussed on urgent tasks. Often time to discuss and undertake case management of chronic conditions or other conditions that could be managed out of a hospital is not available. The skill set of emergency staff differs to that required for ongoing care and management in a home setting.
The second issue is the forecast lengths of stay. Some of the declines in hospital stay have been due to efficiencies, due to better technology and care and have not been dependent on care at home. However, other declines have been driven by post acute care in the home programs. Part of achieving continuing decline in length of stay will depend on the availability of such care. There is an issue as to whether declining stays in hospital should continue to be pushed. For example, costs saved are greatest when an admission is avoided or when many days care is saved. Care costs at the end of a stay in hospital are at their lowest, so the savings are marginal and are not the average cost of a DRG.
Again efficiency and effectiveness need to be considered. For example, while patient satisfaction is generally high with going home on supported care, outcomes may be no better and costs higher. In some cases, confinement in hospital may be important to establish the outcomes desired. For example, very low lengths of stay in maternity units may counter establishment of breast feeding. Women of low socio-economic status who have the poorest rates of breast feeding tend to favour the Domiciliary Midwives Program and leave hospital on days 1 and 2. While it is efficient, effectiveness also needs to be considered.
The forecasts tend to point to the efficiencies that are possible in length of stay, whilst assuming the outcomes are effective. Reducing length of stay for efficiency reasons is valid where health gain is not compromised.
The forecasts also imply:
- A small increase in the number of bed days;
- Overall work will be busier and the acuity of patients higher;
- A large increase in the proportion of same day medical and surgical activity (~71%);
- Requirements of both services and facilities to respond to increasing non inpatient occasions of services, emergency department workload, community health and transitional care;
- That the "busy" nature of work carries with it risks to care continuity and safety.
This future operating environment therefore has a number of implications for SWSAHS such as:
- The need to continue to improve allocative efficiency, eg. networking;
- The need to achieve reductions in length of stay (where outcome remains effective also) to deliver efficiencies and "free up" existing capacity to provide more services (technical efficiency);
- The need to look to flow reversals to improve equity and as a source of funding;
- The need and ability to change work practices;
- There will be people waiting to access services; and
- There will be a need to prioritise allocation of resources and find the balance between those strategies that keep "well" people well, keep people with chronic illnesses stable, minimise the "at risk" population becoming chronically ill, and dealing with acute events and acute complications of existing disease.
11.2 Changes in the Supply of Acute Services
Supply in this section refers to the total amount of activity provided by services inside SWSAHS to both SWS residents and out-of-Area residents. Capture refers to the number of SWS residents treated within SWSAHS. Self sufficiency refers to the number of SWS residents treated within SWSAHS as a proportion of SWS resident demand. This is usually expressed as a percentage. In addition, SWSAHS supplies services to non-SWS Area residents, these are referred to as inflows. Where SWSAHS resident demand exceeds local supply or services are not available, residents access care out of the Area and are referred to as outflows.
Figure 14 summarises the forecast change in the supply of acute services by SWSAHS to 2001 and 2006. This represents the maximum scenario as it includes flow reversals as well as growth of 4% per annum which is currently unfunded.
The following should be noted in regard to Figure 14:
- 3° – refers to tertiary services
- N/T – refers to non tertiary services
- D/O – refers to day only services
- The number of separations is provided followed by the number of bed days in brackets
- Unqualified neonates (well babies) are not included as the APPI model does not include unqualified neonates. This has not been added to maintain a constant base for projected activity. However, other supply information in Appendix D for 1996/97 does include this activity.
Figure 14 – Supply of Acute Services 1996-2006
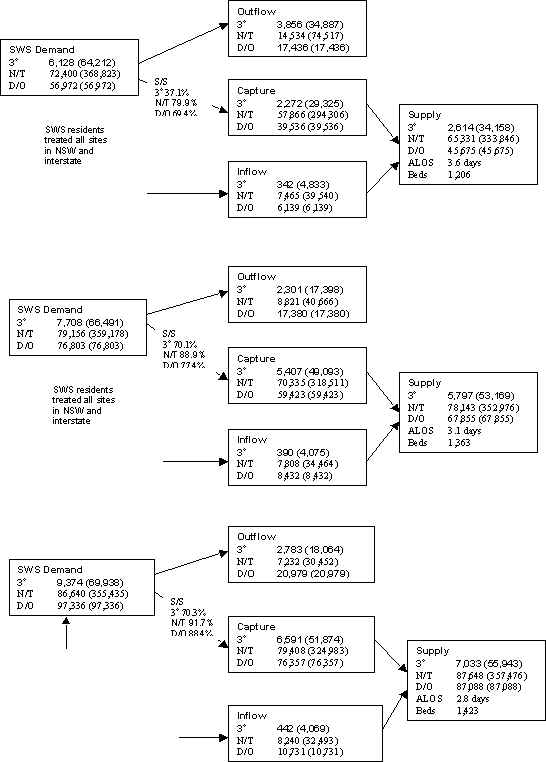
The following main points should be noted from Figure 14:
- Overall self sufficiency targets of 82.6% in 2001 and 84% in 2006;
- The main impact of flow reversal to 2001 is in relation to tertiary services;
- The main impact of flow reversals for the period 2001 to 2006 is in relation to non tertiary overnight and same day services. This would mean that residents of SWS are basically able to access all non tertiary services they require within SWSAHS and all tertiary services excluding those provided only at limited sites. "Natural" flows of patients to geographically closer services, unplanned admissions and ongoing personal choice of service, is assumed to continue;
- There are ongoing reductions in length of stay;
- The current total acute bed capacity in SWSAHS is generally appropriate, although the balance of overnight and day only may need further refinement.
11.2.1 Future Acute Services Staffing Requirements
In relation to future staffing requirements, an estimate has been made based on the number of separations per Full Time Equivalent (FTE) staff.
In 1996, there was 4,138 FTE staff in acute facilities in SWSAHS. This is equivalent to 27.5 separations per FTE. This has increased to 29.3 separations per FTE in 1998/99. Using this ratio would equate to 5,181 FTE staff in 2001 and 6,203 staff in 2006. This would be the maximum staff requirement as this includes growth in workload, as well as flow reversals.
If there was only flow reversal to 2001, this would require an additional 530 FTE staff based on this ratio. If there was no growth from 2001 to 2006 and only flow reversal, this would require 731 FTE staff.
Given the changes forecast in the way that services will be provided in the future, the skills mix of the Area will also need to change to match this. Staff support and development will be major challenges for SWSAHS.
11.3 Supply of Sub Acute and Outpatient Services
11.3.1 Sub Acute Inpatient Services
The sub acute bed self sufficiency in 1996 was 72% with significant inflows. There are currently 154 designated sub acute beds in SWSAHS. It is anticipated that an increase in acute activity provided in SWSAHS as a result of flow reversals and growth in demand will also create demand for sub acute services within SWSAHS, particularly for rehabilitation and palliative care. For example, the increase in availability of neurosurgical services in SWSAHS would be expected to have an affect on the need and type of rehabilitation services.
As there is no planning model (such as APPI) to estimate future demand for sub acute inpatient services, the acute growth rate of 6.7% per annum (including flow reversal and growth of 4% per annum) has been applied to sub acute activity currently being provided within SWSAHS. This results in the number of separations increasing from 2,000 to 3,340 by 2006. At an average length of stay of 20 days and 95% occupancy, 192 beds, or an additional 31 beds, will be required in SWSAHS. Alternative models of care, such as provision of more acute rehabilitation in the home, will have implications for the need for additional beds and where these should be provided.
It would be anticipated that with the projected increase in the number of aged people in SWS, there would be increasing demand for aged care psychiatry services. Braeside Hospital currently has 16 aged care psychiatry beds, Bankstown Hospital has 16 acute beds and there are plans for an additional 8 acute beds as part of the Macarthur Strategy.
The National Strategy for Planning Palliative Care Services 1998-2003 has accepted a UK planning standard of 40-60 beds/million residents. This provides capacity for longer stays of up to 3 months. This would equate to a need for between 31-47 beds in 2001, increasing to 33-50 to 2006 for SWSAHS. There are currently 27 palliative care beds in SWSAHS with a total of 30 planned with the additional 3 beds as part of the Macarthur Strategy. This would require up to 20 additional palliative care beds by 2006.
11.3.2 Mental Health Services
SWSAHS currently have 90 psychiatric beds operating at 70% occupancy. Based on demand assumptions of a 4% growth per annum in admission, no decline in length of stay and 90% occupancy, the forecast bed requirement to 2001 is 75 beds and 88 beds in 2006.
While the APPI model suggests no additional mental health beds are required to 2006, the NSW Health Centre for Mental Health bed planning suggests that the Liverpool/Fairfield Sector is significantly under bedded. Access to inpatient services for SWS residents is limited, so current utilisation of services is not a good indicator of actual need for the service. Planning will therefore continue to determine the number of additional inpatient beds, ambulatory care and other community based services required.
SWSAHS currently receive only 5.2% of the Mental Health funds through the RDF. The equitable share of resources is 9–10%. These resources would be invested in Liverpool/Fairfield Sectors.
As well as these workload and funding issues, there are a number of issues that affect how mental health services will be provided in the future and which will need to be incorporated in any future service development.
The Second National Mental Health Plan (1998) notes that people with a mental illness are still disadvantaged in society as a result of stigma, discrimination and lack of available and appropriate services. The plan identifies the need to improve health outcomes for people with a mental illness and outlines three key platforms:
- Prevention, promotion and early intervention
- Partnerships
- Quality and effectiveness
These three platforms are integral to Caring for Mental Health: A Framework for Mental Health Care in NSW (1998) which outlines six strategic directions for the development of mental health services in NSW. These are:
- Working together for better mental health – developing partnerships
- Emergency mental health response
- Mental health promotion, prevention and early intervention
- Providing better mental health care
- Quality and effectiveness in mental health care
- Putting the building blocks in place
The National Health Plan and Caring for Mental Health expand the focus of mental health services and emphasise the need to provide mental health services for people across the lifespan and across the spectrum of intervention, that is, prevention, promotion, early intervention, treatment, support and maintenance. This encompasses the provision of services to people with a broader range of mental disorders such as anxiety related disorders and personality disorders.
This expanded focus has implications for allocation of resources and reinforces the need for a collaborative approach to care across a range of health and human service providers, for example with General Practitioners.
11.3.3 Non Inpatient Hospital Services
If there is 6.7% per annum increase within SWSAHS (including 4% per annum growth and flow reversals) in hospital separations, NAPOOS for hospital non inpatient workload will increase by 314,000 by 2006. This assumes no shift of service delivery towards avoiding admission and managing as outpatients.
Based on past trends, a 50% growth in emergency attendances and a 73% growth in admissions is forecast. The growth in emergency activity is very high and requires specific attention as this is a significant point of access to the hospital system
Given the significant increase in this volume of activity, each service with an outpatient function will need to carefully plan its future workload. Current forecasting would suggest that there will need to be an investment in the style and model of service and potentially in physical facilities to ensure they are capable of handling the workload.
11.3.4 Community Based Services
An increased workload from 883,574 to 1,003,009 OOS has been estimated related to population growth. The breakdown of "community health" used in the above figures is:
|
682,000 |
|
58,000 |
|
143,000 |
There is an issue for Primary Health Nurses (PHN) as the shift of activity from inpatient to community settings will increase the workload for PHNs, as well as the increase due to population growth. For example, the PHN OOS is 20–25% of all Primary and Community based OOS. Post acute care is currently a small proportion of total workload. It is possible that in future 50% of all PHN workload will be non acute. This will double their workload and increase Primary and Community based OOS to 850,000. The adjusted total OOS would then move to 1,050,000 OOS if this PHN workload shift were possible immediately. Applying population growth of 13.6% by 2006 gives total OOS of 1,192,000. This is an increase of 310,000 OOS.
As well as the increase in workload that has been forecast, there are a number of other issues that will affect community based services in the future:
- Better information will be collected and available to measure community health and its health outcomes. This will provide a better foundation to plan and develop community health services;
- The introduction and expansion of evidence based practice in community health will inform and assist in determining the optimal configuration of services. For examples, initiatives such as Families First will assist in identifying what services should be provided and how best to do this to meet the needs of children and their families;
- There will be an increase in the number of more acute patients being managed and cared for in the community. This has implications for the skills, training and support required for staff, as well as the hours of operation of services (for example, 24 hour back up services);
- Ongoing development of partnerships with other government and non government agencies; and
- Greater integration of services between providers with multidisciplinary approaches and sharing of skills and expertise. Opportunities and benefits of physical collocation of services provided by Councils, the Area Health Service and agencies such as the Department of Community Services, should be considered.
11.3.5 Future Non Acute Staffing Requirements
There will need to be investment in PHN numbers if this workforce is to be the key supporters of the increased post acute care service delivery required to continue to reduce inpatient length of stay. This will require significant investment. As indicated, investment will be required in ensuring staff have the necessary skills, training and support to provide this care.
An increase of 310,000 OOS by 2006 would equate to an additional 231 PHNs based on a 7 day 12 hour day service. There may also be implications for other allied health and medical staff to support this shift and growth of activity in the community.
12. SWSAHS Objectives
The purpose of the AOP is to assist in achieving the following objectives for SWSAHS. These are key challenges 3,4 and 5 of the Strategic Directions Statement, and are the core of the changes we need to make regarding our services:
- Equity
- Efficiency
- Effectiveness
- Acceptability
Table 10 summarises the main issues arising from the analysis of SWSAHS’ current operating environment and forecast changes in health care. These have been linked to each of the Area’s four objectives. These issues are discussed in more detail following the table.
Table 10 – SWSAHS Objectives
| Objective | Strategies | Target |
| Equity | Flow Reversal |
|
| Geographic equity |
|
|
| Program share equity |
|
|
| Efficiency | Networking |
|
| Benchmarking |
|
|
| Integrated care |
|
|
| Achieve reductions in inpatient length of stay where effective |
|
|
| Increase day only and ambulatory services as appropriate |
|
|
| Set efficiency targets |
|
|
| Effectiveness
Defined for SWSAHS as doing the work to achieve the most health gain |
Decisions on investments made with regard to evidence of effectiveness |
|
| Increase the use of underutilised effective intervention and decrease the use of over used ineffective interventions |
|
|
| Implement evidence based practice |
|
|
| Acceptability | Inform the community of how health care be in the future |
|
| Involve the community in decision making regarding relative investment |
|
12. Why Equity is Important
Greater equity is considered important for SWSAHS for the following reasons:
- Improved access to services. This includes screening and diagnostic services so that earlier diagnosis and treatment is achieved with reduced morbidity and mortality. It has been demonstrated that distance from services, such as radiotherapy, influence patient’s decisions to proceed with treatment and utilisation of services and may delay detection;
- That residents are able to receive the same level of care regardless of where they live in SWS or where they access services;
- The population characteristics of SWS residents indicate potential barriers to accessing out-of-Area services. Provision of services locally assists in overcoming barriers such as the cost and availability of transport, the cost of family dislocation and travel, the ability to attend services as an outpatient; and the ability to successfully connect the patient back into local services;
- Specific groups in SWSAHS, such as low socio-economic status, refugees, Aboriginal and Torres Strait Islanders and people with disabilities or participation restrictions, may be particularly disadvantaged in accessing services. This requires development of strategies that ensure equitable access to services;
- Residents with mental health needs can access the care and support services they require within SWSAHS;
- Reductions in length of stay (LOS) due to greater ability to attend services such as pre admission clinics and perioperative early morning services and connecting with local community services for post acute care;
- Flow reversals for acute inpatient services potentially deliver an estimated $47 million to SWSAHS by 2001. This includes adult and paediatric flows. This would enable funds to be directed toward high priority areas for the population and for services to be developed consistent with changing trends in care and efficient practices;
- Makes efficient use of existing infrastructure, which has the capacity to treat SWSAHS residents locally;
- The targeting of flow reversals is an approach where funds are "created" by avoiding payment to other Areas for treating SWS residents. By providing services more efficiently than other Areas, more services can be provided in SWSAHS than could have been "purchased" outside.
An important element of greater equity is flow reversals, where SWS residents are able to access services within SWSAHS. This does not mean treating all SWS residents as there will always be people who receive care outside the Area for emergency services, through personal choice and where some selected statewide specialty services such as liver, pancreas and heart/lung transplantation, are not provided locally.
Should SWSAHS make no effort to reverse flows, and even if funded to do the extra forecast activity, SWSAHS’s position in regard to self sufficiency worsens from 73.6% to 72.9% by 2006. Equity is therefore not improved. The 1996/97 self sufficiency in tertiary services was 37.1% but decreases to 35% in 2006. The self sufficiency in non-tertiary and day only services is 75.3% in 1996 but would fall to 74.8% in 2006.
The APPI forecasts show that if SWSAHS makes no effort to influence flow patterns, outflows keep growing. SWSAHS has demonstrated the ability to achieve flow reversals with tertiary self sufficiency 47.4% and non tertiary self sufficiency of 76.4% in 1997/98. SWSAHS has therefore already made significant progress in achieving greater self sufficiency as well as meeting growth in local demand for services.
The cost of the outflow at the NSW Health default price of $2,300 grows by nearly $4 million per annum over 10 years. The major contributor to outflow cost by 2006 with no change in supply is tertiary outflow.
As part of a strategy of targeting specific outflows which can be reversed, the following services with high demand, high outflows with a high number of planned admissions and low self sufficiency are considered to have first priority because of their potential for achieving flow reversal. It should be noted that these services are acute inpatient services and there is limited information available for services that are predominantly ambulatory or provided in the community.
In regard to tertiary services, the following seven SRGs comprise most of the demand for tertiary services (72%) and outflows (72%):
- Cardiology
- Cardiothoracic surgery and bypass
- Neurosurgery
- Haematology
- Respiratory medicine
- Vascular surgery
- Perinatology
For non tertiary overnight services, the following services have been highlighted due to a combination of factors including high demand, outflows with a significant number of planned admissions and low self sufficiency:
- Cardiology
- Gastroenterology
- Neurology
- Renal medicine
- Respiratory Medicine
- Gynaecology
- Orthopaedics
- Urology
Same day services with high demand and relatively low self sufficiency include:
- Gastroenterology, including gastroscopy and colonoscopy
- Medical oncology
- Renal Dialysis
These services are being subject to a service analysis process that will determine how they will be provided across the Area.
13.1 Service Analysis Process
For the priority acute service streams that have been identified, the following service analysis process will be undertaken. This has been completed for trauma and elective (joint) orthopaedics, urology, neurosciences, cardiology and cardiothoracic surgery and gastroenterology This process will be undertaken for each service stream.
Each service will be considered in the context of the Area-wide provision of the service and will include the following analysis:
- Analysis of current workload including public and private sector,
- Detailed analysis of current and future demand for the service including outflows, capture and inflows by Diagnostic Related Group (DRG). This is also undertaken by Sector Health Service;
- Detailed analysis of the supply of the service within SWSAHS and by Sector Health Service;
- Consideration of tertiary, non tertiary and day only activity;
- Analysis of outflows and estimated flow reversal;
- Cost analysis;
- Recommendations regarding service provision and organisation.
As indicated, each service analysis will include recommendations regarding the service. These will be initially considered by the Acute Services Reference Group and then will form the basis for consultation with the service providers to develop an implementation plan and time frame. These will over time be included in the AOP.
13.2 Program Share Equity
There has been a shift in the relative share of the program budgets in SWSAHS with an increasing percentage of the budget being allocated to primary and community based and outpatient services. What remains unclear is how best to determine the future shares of the budget which is generally historically based.
14. Why Efficiency is Important
In an environment where the level of resources provided to SWSAHS is unlikely to meet the forecast increase in demand for services, efficiency is a major factor in being able to make available resources go "further" and giving the Area some ability to allocate resources to new or expanded services.
Efficiency is also an important issue in flow reversal. If flows are reversed, but the services are not provided at or below average costs, then we will manage them at a financial loss. If SWSAHS develops better processes in providing these services, then what we pay other Areas today will buy more of our own local service in future. It may also mean that where the service is provided more efficiently by other Area Health Services than SWSAHS, then SWSAHS may continue to purchase this service outside the Area.
Efficiency may be improved by better care processes and building on service networks that currently exist within SWSAHS. There is a real advantage in developing clinical networks that allow the majority of non-tertiary work to be managed within those sectors with lower infrastructure costs. This would ensure that the higher infrastructure costs at Liverpool Hospital associated with tertiary services is directed predominantly to tertiary work.
SWSAHS must consider ways to generate efficiencies and "free up" resources to invest in priority areas. The two main options to generate efficiency are considered to be:
- A shift of activity from overnight to day only;
- Networking of services with distribution of services consistent with the efficient providers of the service.
It is anticipated that the Service Analysis process will have a significant role in identifying the options that will assist in these two areas.
Integrated care is also an important part of improving efficiency. By supporting shared care with GPs and developing continuum of care processes, the Area can seek to improve and streamline the management of patients in the health care system.
14.1 Ambulatory Care
Consistent with changes occurring in the provision of health services, it is forecast that same day activity will continue to increase. Based on no change in SWSAHS’s supply of services, it is estimated that there will be a 41% increase in activity levels over the 10 year period from 1996 to 2006. However, the same day workload increases by 71.5%, tertiary workload increases by 42.5% and non tertiary workload increases by 20.1%.
Due to declining length of stay, it is estimated that while hospitals will be much busier, there is not a requirement to increase overnight beds. This does mean however, that the relative distribution of beds between overnight and same day needs to be considered as well as how this large increase in ambulatory care can be achieved. There is a risk that if this is not achieved, there will be insufficient capacity to meet demand.
Ambulatory care has a number of components that may include: transitional care; hospital in the home; day surgery/medical; supported discharge; and ambulatory assessment including day hospital. Models of care which support Sector Health Service objectives need to be further developed and enhanced.
In regard to the more acute component of ambulatory care, the initial focus should be on day medical services, with consideration of opportunities for day surgical services at all sites. Ambulatory mental health services also require consideration.
Another important aspect of ambulatory care is managing the increase in activity at Emergency Departments (ED). Developing care processes that prevent people representing or having multiple attendances will be will be an important issue.
Ambulatory care is important for a number of reasons which may include: it provides an alternative model and "frees up" hospital capacity for managing the forecast increase in activity; it reflects changing clinical practice; it may be more cost-effective than an overnight hospital stay; and it reduces the risks associated with overnight hospitalisation.
There are issues with current funding arrangements that need to be considered in relation to increasing ambulatory care. As an example, private health funds do not fund hospital in the home. In addition, the increasing acuity and complexity of community care may not be adequately reflected in the current estimated cost of a non inpatient occasion of service and there may be financial incentives to admit people for care.
Fairfield, Liverpool and Bankstown are considered key sites to further develop ambulatory care models. Macarthur has made significant progress in developing an Ambulatory Care Model.
15. Why Effectiveness is Important
Effectiveness is about providing health benefit and is fundamental in the objective of maximising health or health gain. It means making decisions on allocation of resources based on the best available evidence. It also means taking an evidence based approach on a population basis and across the care continuum.
Health improvement, or health gain, is defined as "a change for the better in the health of an individual or in the health status of the population" (NSW Health, Health Improvement Plan Guidelines, March 1997). The notion of health improvement opens up opportunities to consider a wide range of activities, other than direct service provision, to improve the health of populations.
SWSAHS aims to ensure that this is achieved by a range of approaches including:
- Ensuring ongoing assessment of population health needs;
- Making investment decisions based on the evidence of effectiveness and increasing the use of underutilised effective interventions and decreasing the use of over used ineffective interventions;
- The Priority Areas providing the direction for service development and identifying care processes that maximise health gain;
- Completing service plans for the 11 Priority Areas;
- Considering the implications of clinical disciplines where significant demand is forecast and developing an appropriate response;
- Considering the evidence regarding the effectiveness of services or interventions;
- Organising and managing services to support health improvement objectives;
- Improving the integration of care with other services. For example, shared care for diabetes and mental health, improving referrals from General Practitioners to Emergency Departments and improving discharge processes and information;
- Implementing already agreed evidence based treatment guidelines and protocols.
Given the increase in demand which is forecast, there are real opportunities to change the future by focussing on strategies that keep "well" people well, keep people with chronic illnesses stable and minimise the "at risk" population becoming chronically ill. As well as being more effective in achieving better health for the SWS population, this will also mean resources are used more efficiently and equity is achieved because we will be doing the "right thing" on the "right people" and only when it is needed.
16. Why Acceptability is Important
Both informing and engaging the community in decision making will assist in achieving the significant changes in the way that health services will be organised and delivered in the future. The community includes SWSAHS staff, General Practitioners, Nursing Home operators and other service providers, as well as the general community. All these groups are key in gaining acceptance of, and achieving, change in health care.
Community acceptance of alternative care models and increasing care being delivered in the home is essential if this shift in the care setting is to be achieved. Different approaches to involving the community will be necessary due to the varied demographics in SWSAHS.
This community involvement is very important in an environment of limited resources. Choices need to be made. An informed community can assist health professionals make choices with the community. A community consultation policy is being developed for consideration by the Area’s Board.
Trying to satisfy the differing objectives of equity, efficiency, effectiveness and acceptability may result in some areas of disagreement. For example, why increase efficiency to respond to increased demand for a service which does not lead to an improved health outcome. The service may have also a high community acceptability and not allocating additional funds may cause concern. This demonstrates the importance of considering all the Area’s objectives in determining overall priorities.
The 11 Priority Areas and their associated Advisory Committees are an important way of informing the Area Health Service on the most appropriate way to achieve these four objectives.
17. Future Hospital Roles and Distribution of Acute Capacity
17.1 Hospital Roles
While there will not be any significant changes in role levels to 2001, there will be a focus on delivery of acute services as part of an Area network and development of high quality services consistent with their role delineation.
Liverpool Hospital will continue to be the Area’s tertiary referral centre. Where components of tertiary services are developed at other hospitals, such as back and neck surgery, these will be networked to the tertiary "hub" at Liverpool. Liverpool will also continue to provide some district level services consistent with servicing its local catchment.
Bankstown Hospital will continue at predominantly level 5, Fairfield predominantly level 4, Macarthur mainly level 4/5 and Bowral mainly level 4. While each hospital will provide district level services for its local catchment, there may be changes in the current distribution of services and the development of "centres" for particular services at specific hospitals.
17.2 Distribution of Acute Capacity
If there was no change in the current workload of SWSAHS facilities, that is no flows were reversed and no additional services were supplied, the number of beds required in 2001 and 2006 to deliver the current number of hospital separations would fall significantly due to the effect of falling length of stay.
For example, in 1997/98, 125,144 separations and 423,381 bed days were supplied by SWSAHS services. The average length of stay was 3.4 days. If the same number of separations were provided in 2001 and 2006, but at the estimated length of stay in these years, 387,946 and 337,889 bed days would be required in 2001 and 2006 respectively. This equates to approximately 1,180 beds in 2001 and 1,028 beds in 2006 (at 90% occupancy).
There are currently 1,470 average available beds in SWSAHS facilities (including rehabilitation and mental health). Using the 1998/99 average available beds for Macarthur and built beds for the remaining SWSAHS hospitals, there is approximately 1,716 beds built beds (including bed spaces not staffed or equipped). At the completion of the Macarthur Sector Strategy in 2003, there will be 1,850 built beds. If SWSAHS workload remained the same, this would suggest that there are 536 beds in 2001 and 822 beds in 2006 potentially "spare" as a result of falling length of stay.
It should be noted this does not mean that these beds are immediately available, while some areas would require refurbishment to make the spaces appropriate for use. Some of this capacity would also be required for additional mental health and rehabilitation services.
If only the forecast 4% per annum growth in demand to 2001 was met (that is, there was no flow reversal), compared to the current average available beds, SWSAHS would need 3 less tertiary beds, 35 less non tertiary overnight beds and an additional 31 same day beds. This reflects the impact of increasing ambulatory care and reductions in length of stay.
If only flow reversals as forecast were met by SWSAHS by 2001, an additional 58 tertiary beds, 93 non tertiary overnight beds and 13 same day beds would be required. This is due to the impact of flow reversals in tertiary services to 2001. The impact of ambulatory care and reductions in length of stay is far less due to the influence of greater tertiary work being performed in the Area. The proposed flow reversal to 2001 requires 164 acute beds. As demonstrated this can be accommodated within SWSAHS’s physical capacity.
The main conclusion that should be drawn from this analysis is that no overall increase in physical bed capacity will be required in SWSAHS to 2006. This does mean that there needs to be attention to achieving ongoing reductions in the length of inpatient stays.
Looking further ahead to 2006, the future number and distribution of acute beds needs to:
- Accommodate the forecast flow reversals;
- Include the additional 81 acute beds agreed as part of the Macarthur Strategy (comprising 43 same day and 38 non tertiary overnight beds),
- Include the reversal of district level activity from Liverpool to Macarthur;
- Reflect the outcomes of service networks;
- Enable the achievement of reductions in length of stay and increases in same day activity;
- Provide flexibility in beds allocated to accommodate the initial phase of flow reversal to 2001, the timing of the additional Macarthur beds and the uncertainty of funding to meet the 4% per annum growth in demand.
Overall, the total SWSAHS built bed capacity required is adequate for the activity forecast. However, consistent with expected increases in day only activity, some reallocation between overnight and same day is required.
As demonstrated, the net effect of both growth in demand being funded and flow reversal being successful, is that an additional 58 tertiary beds, 58 non tertiary over night beds and 44 same day beds to 2001 as an absolute maximum. This has the following implications for each hospital in SWSAHS:
- This would be considered to be the maximum number of beds as growth is included which is not yet funded;
- There are currently 1,470 average available acute beds in SWSAHS with greater built capacity. This activity can be accommodated from existing built capacity;
- While there is no increase in overall bed capacity at Liverpool, tertiary activity would be increased at Liverpool, effectively requiring an additional 2 wards. This will result in an increase in the number of tertiary beds relative to non tertiary overnight;
- The Macarthur Strategy will reverse approximately "1 wards" worth of district activity from Liverpool providing a strategy to reduce non tertiary capacity after 2003;
- The non tertiary overnight beds required in SWSAHS are met by the Macarthur Strategy but at a later time than 2001. If these beds are opened then these will need to be "shut" post Macarthur. If required, these would be opened at Fairfield. Alternatively an increase in occupancy rate could be a strategy to provide this capacity in the interim rather than opening beds;
- Same day capacity needs to be increased at Liverpool, Bankstown and Fairfield. Again no increase in capacity is required but conversion of overnight beds to same day beds will be necessary. This may also require some refurbishment of existing facilities;
- Bowral Hospital will continue to provide a district level service consistent with its local catchment.
It is more difficult to estimate the bed requirement of the activity forecast to 2006. However, as the flow reversal effect from Macarthur will be in non tertiary activity, the main impact is a requirement for greater same day capacity as trends in ambulatory care and shorter lengths of stay are forecast to continue. This reinforces the need for greater same day capacity at Bankstown, Liverpool and Fairfield.
The forecast bed day capacity needs to be considered against the projected increase in throughput. For example, reductions in length of stay in clinical specialties that currently exceed comparative benchmarks, coupled with the current bed supply, may fully or partly accommodate projected increases in bed day requirements. Changing clinical practice where some clinical specialties have been included in the forecasts but will be no longer provided in hospitals would also have a significant impact.
17.3 Number of Operating Rooms
As indicated, based on a combination of surgical activity and endoscopy procedures, 34,743 Episodes of Care (EOC) were supplied in 1997/98 in SWSAHS. A per session workload of 3.5 cases has been estimated based on dividing operating room activity by the number of funded sessions per year of 9,820 (assuming 2 sessions a day and a theatre year of 10 months duration).
The forecast surgical flow reversal to 2001 is equivalent to 3,722 EOC. The growth in surgery forecast up to and including 2001 is 8,062 EOC. The current capacity of 4,180 sessions per year would accommodate growth in demand for 2001, flow reversals and provide capacity for 2,846 EOC of the 2006 surgical growth forecasts without the need for additional operating theatres.
Assuming no major shift in the non-surgical management of conditions currently requiring a surgical procedure, the remaining forecasted growth in surgery to 2006 of 5,641 EOC would require an additional 1,611 sessions per year. In this case, SWSAHS would require the equivalent of 4 operating theatres.
The Macarthur Strategy results in 3 additional operating theatres by 2003. Session capacity equivalent to 1 operating theatre would therefore be required to 2006.
In light of this modest increase, it is considered that work practice redesign could provide this capacity without the need to build additional operating rooms. Operational practice is a major factor in on operating room utilisation. For example, provision of an additional session through extended hours of operation would increase capacity significantly. The assumptions used to estimate the future requirement are considered conservative and give some margin for error. However, should additional operating rooms be required, 1 would initially be provided at Fairfield Hospital.
17.4 Distribution of Sub Acute Inpatient Capacity
As indicated in section 11.3.1 it is considered that there is some requirement for additional inpatient capacity for palliative care and rehabilitation services.
It is suggested that beds are identified in Liverpool and Bankstown Hospitals for patients requiring admission for acute palliative care services, such as radiotherapy, awaiting discharge to a palliative care unit, anaesthetic procedures for pain or for palliative care emergencies such as spinal cord compression.
Beds offering longer term palliative care are required in all Sectors. However, this may involve options such as contracting with the nursing home sector.
If length of stay falls due to programs such as home based rehabilitation, then there may be less of a requirement for inpatient hospital beds for rehabilitation. Any additional beds required for sub acute inpatient rehabilitation services would be considered initially for Fairfield (Braeside). However, the optimum distribution of sub acute, as well as acute rehabilitation services will be further considered.
Requirements for acute and community aged care psychiatry services will need to be further considered as it would be expected that demand for these services would increase with an ageing population. There are currently no services in Macarthur or Wollondilly, while there are some difficulties within existing hospitals in managing patients with behavioural disturbances or those who may wander due to dementia or other forms of brain damage.
18. Possible Sources of Additional Funding
The Area will continue to seek extra funding for SWSAHS (in 1999 $ and cost structures) as follows:
Achievement of SWSAHS’s Resource Distribution Formula 2001 target – this is equivalent to $18 million. This amount changes annually as budgets of Areas change and reflects current flow patterns
Achievement of an equitable share of mental health funding – this is equivalent to $17 million
Flow reversal. This has been estimated to be $47.35 million to 2001 with a further $15.8 million to 2006.
Growth funding – the cost of growth in demand is estimated at approximately $40 million to 2001
19. Summary of Key Issues to 2006
Table 11 summarises some of the main issues arising in the future. While asset issues are being addressed through the Area’s Integrated Asset Strategy, some possible physical asset implications have been included:
Table 11 – Key Issues to 2006
| Self sufficiency | Targets of 82.6% and 84% in acute services in 2001 and 2006 respectively | |||
| Roles of acute facilities | Essentially unchanged, but development of "centres" consistent with acute service networks. Liverpool Hospital continues as the Area’s tertiary referral centre. | |||
| Acute bed capacity | No overall increase in capacity. However, there will be an increase in tertiary beds at Liverpool and an increase in day only at Bankstown, Liverpool and Fairfield. | |||
| Sub and non acute bed capacity | An increase in capacity is required. To be achieved within existing bed capacity but with potential increases at Fairfield (Braeside) considered initially as well as the appropriate Area wide distribution of beds. | |||
| Length of stay reductions | Year |
Tertiary |
Non tertiary |
|
1996 2001 2006 |
13.1 days 9.2 days 8.0 days |
5.1 days 4.5 days 4.1 days |
||
| Acute staff numbers | Flow reversals to 2001 and 2006 would require 530 and 731 additional FTEs respectively. Flow reversals and growth to 2001 and 2006 would require 1,043 and 1,022 additional FTEs respectively. | |||
| Non acute staff numbers | It is estimated that 231 PHNs would be required to 2006. This does not include additional allied health or medical staff. Additional staff for non acute inpatient services would be achieved through reallocation of existing staff as beds were substituted. | |||
| Ambulatory care | Significant
attention to ambulatory care is required to achieve the length of stay reductions forecast
and achieve benchmarks in day surgery. NSW Health goal of 60% of all surgery on a same day basis by June 2000/01. |
|||
| Operating rooms | Potentially 1 additional room would be required. This could be achieved through work practice redesign or a change in operational practices. Alternatively a room could be provided at Fairfield Hospital. | |||
| Networking | Development of Area wide services as required and networking of appropriate services across the Area will be supported. | |||
| Demand management | Management of the overall forecast increase in demand, as well as the specific areas identified as being high demand areas (for example, emergency department, renal dialysis), will be key in becoming more proactive and developing strategies that in fact reduce demand on health services. | |||
| Human Resources | Strategies to
recruit appropriately skilled staff to provide services, including the increase in
services proposed as part of the Macarthur Strategy, will be required. Training, education and support for staff will be required to achieve work practice change and respond to the changing provision of health services. |
|||
| Mental Health | This will be a major issue in both improving SWSAHS’s share of current NSW mental health resources and capital works. | |||
| Evidence based practice | Decisions will be made based on the best possible evidence available of effectiveness and appropriateness. Where this is not available, strategies will be required to evaluate interventions and services. | |||
| Communication | Communication will be essential to achieve the changes in the organisation and provision of health care that is forecast | |||
| Asset issues | An Area Asset
Strategy is being developed. However, major asset issues include:
|
|||
20. Area Operations Strategy
There are two main phases in the Area Operations Plan to 2006.
Phase 1: Actions to December 2002
This phase addresses the three and a half years 1999/00, 2000/01, 2001/02 and the first 6 months of 2002/03. The significant components in phase 1 involve the following:
- Completion of service analyses for each acute clinical service stream to progress networking of services as appropriate;
- Investment in local acute service enhancement through reversing outflows for acute services. This phase will have a flow on effect on non acute inpatient care, outpatient care and community based care;
- Enhancement of ambulatory care services at all sites;
- Initiation of strategies to address the deficiencies in resourcing of all aspects of mental health care;
- Development of Asset, Human Resource and Information Technology Strategies to support the AOP;
- Development of a communication strategy to engage our staff and the community as partners in considering changes in health care.
Phase 1 will require:
- Acute flow reversals;
- Designing a response to the flow on effects to non acute services;
- Improvement in SWSAHS mental health resource share;
- Achievement of SWSAHS RDF 2001 target share;
- Investment in transitional care and home care;
- Underpinning of service changes with primary and population investments aimed at long term health improvement in the population;
- Alignment of acute and non acute inpatient capacity consistent with changes in service delivery, flow reversals and funding for growth in demand.
Phase 2: From January 2003
While phase 2 largely involves the Macarthur Strategy, Macarthur will contribute to flow reversals in phase 1 through the agreed service networks. However, its main effect will be from mid 2003 when Campbelltown Hospital opens at upgraded levels of service and with additional bed capacity. This will contribute to reversal of out-of-Area flows as well as enable further tertiary growth at Liverpool by reversal of flow of Macarthur residents from Liverpool back to Macarthur (intra-Area flow reversal). This phase will also continue flow changes commenced in phase 1.